"DISH" is a type of degenerative arthritis which is characterized by flowing calcifications along the vertebrae of the spine. It is commonly associated with inflammation (tendinitis) and calcification of tendons at their attachments points to bone. This also leads to formation of bony spurs. Marked calcification and ossification of paraspinous ligaments occur in this disease. Although it is characterized as a variant of Osteoarthritis, diarthrodial joints are not involved. Ligamentous calcification and ossification in the anterior spinal ligaments give the appearance of "flowing wax" on the anterior vertebral bodies. However, a radiolucency may be seen between deposited bone and the vertebral body, differentiating DISH from the marginal osteophytes in spondylosis. Intervertebral disk spaces are preserved, and sacroiliac and apophyseal joints appear, helping to differentiate DISH from spondylosis and from ankylosing spondylitis, respectively.
DISH occurs in the middle-aged and elderly and is more common in men than in wome. Patients are frequently asymptomatic but may have musculoskeletal stiffness. The radiographic changes are generally much severe than might be predicted from the mild symptoms.
Signs & Symptoms
The signs and symptoms you experience depend on what part of your body is affected by diffuse idiopathic skeletal hyperostosis. The upper portion of your back (thoracic spine) is most commonly affected. Signs and symptoms may include:
Stiffness in the spine. Stiffness may be most noticeable in the morning.
Pain in the spine. You may feel pain when someone presses on your spine. Not everyone with diffuse idiopathic skeletal hyperostosis in the spine will experience pain.
Loss of range of motion in the spine. Loss of lateral range of motion may be most noticeable. You flex your spine laterally when you do side stretches, for example.
Diffuse idiopathic skeletal hyperostosis in other parts of your spine or other parts of your body may cause stiffness and pain. Additionally, diffuse idiopathic skeletal hyperostosis in your neck (cervical spine) may cause difficulty swallowing or a hoarse voice.
Frequency
According to study [Rothschild, 1985]
Approximately
Men 19%
Women 4%
in population older than 50 years
Imaging Studies
Thoracic vertebrae are involved in 100% of affected individuals, lumbar vertebrae in 68-90% of these persons, and cervical vertebrae in 65-78% of affected individuals. Ligamentous ossification affects both sides of the lumbar vertebral column but tends to be unilateral in the human spine. Prominence of DISH on the right lateral aspect of the thoracic spine is apparently related to aortic pulsations. Left-sided overgrowth is much reduced, also probably because of the influence of aortic pulsations, an idea supported by the notation of left-sided prominence in individuals with situs inversus (left-sided thoracic aorta).
The earliest sign of DISH appears to be new bone formation adjacent to the midportion of the vertebral body, a phenomenon often below the limits of radiologic detection. Recognition of DISH is facilitated by its separation from the body of the vertebrae. This gives rise radiologically to the appearance of a radiodense line paralleling the longitudinal axis of the spine but separated by a clearly definable space.
The general term DISH emphasizes that the ligamentous ossification phenomenon is not limited to the spine. Exuberant ossification at sites of tendon, ligamentous, or joint capsule insertion (enthesitis) is strongly suggestive of the diagnosis. A tendency toward such ossification at any site of ligament and perhaps tendon insertion appears to exist. Enthesial reaction at the iliac crest and ischial tuberosities often is referred to as pelvic whiskering and typically is quite exuberant. Such whiskering was noted in two thirds of iliac crests studied and in 53% of ischial tuberosities. Enthesial reaction was noted in 42% of lesser and 36% of greater trochanters of the femur. Enthesial spurs at the site of insertion of the quadriceps mechanism into the patella were present in 29% of patients studied. Osseous bridging of fibula and tibia was noted in 10% of patients. Distal metacarpal and phalangeal capsular hyperostosis were present in 13% of patients with DISH (Rothschild, 1985).
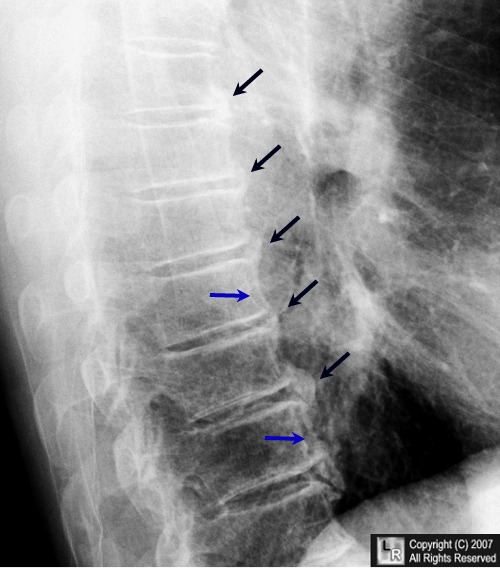
Diffuse Idiopathic Skeletal Hyperostosis (DISH). There is flowing ossification (black arrows)that spans more than four contiguous vertebral bodies while the disc height is maintained andthe flowing ossification is separated from the anterior aspect of the vertebral body (blue arrows).
Complications
- Overgrowth of ligamentous calcification could impinge on other structures (eg, the esophagus). Reports of this are rare and often represent inadvertently discovered, neurologically mediated swallowing deficits.
- Posterior longitudinal ligament ossifications may impinge on the spinal cord on rare occasions.
- Reduced vertebral column flexibility predisposes to vertebral fracture.
Differential Diagnosis
Ankylosing spondylitis
Has involvement of SI joints
Syndesmophytes are thinner
Degenerative disc disease
Osteophytes form only at corners of vertebral bodies
Narrowing and desiccation of disc
Acromegaly
May produce osteophytes but they are not flowing
Fluorosis may produce osteophytes, whiskering and ligamentous ossification
But all bones are uniformly increased in density
Treatment
Because areas of the spine and tendons can become inflamed, anti-inflammatory medications (NSAIDs), such as ibuprofen and Naproxen, can be helpful in both relieving pain and inflammation of DISH. It is hoped that by minimizing inflammation in these areas, further calcification of tendons and ligaments of the spine leading to calcific bony outgrowths (osteophytes) will be prevented.




